|
|
 [Definitie:] "An ergogenic aid is any substance or phenomenon that enhances performance."
(Wilmore and Costill)
[Definitie:] "An ergogenic aid is any substance or phenomenon that enhances performance."
(Wilmore and Costill) 
|
|
|
||
|
||
|
2 8 - 0 2 - 2 0 0 5 Gluteal mass in a bodybuilder: radiological depiction of complication of anabolic steroid use
Khalid Al-Ismail, William Torreggiani, Peter Munk, Savvas Nicolaou
We report an unusual case of a 39-year-old recreational bodybuilder who developed a large painful soft tissue mass in his gluteal area. Radiological imaging with ultrasound, CT and MR imaging demonstrated an inflammatory mass in association with calcifications and fat locules. Biopsy, culture and surgical debridement revealed massive inflammation with acid-fast organisms and granulomatous reaction. The visible fat locules represented lipid used to suspend the anabolic steroid preparation. While local infection is well recognized at the site of steroid injection, this case is unusual in that multi-modality imaging not only helped to characterize the mass, but also showed direct evidence revealing the underlying cause of the mass being depot steroid injections.
Case report A 39-year-old bodybuilder presented to the emergency department with a large tender left-sided gluteal mass that had been enlarging over a 3-week period. He had a history of intermittent anabolic androgen use over the previous 4 years. His regimen consisted of the intramuscular injection of Sustanon (Organon, UK) 250 mg/week, as part of a 12-week cycle (6 weeks on followed by a 6-week gap). Sustanon 250 is an oil-based injection containing four testosterone compounds: testosterone propionate, 30 mg; testosterone phenylpropionate, 60 mg; testosterone isocaproate, 60 mg; and testosterone decanoate, 100 mg. The patient consistently alternated injections between both gluteal regions. He described using a sterile technique, employing new needles (25 G, 1.5 in. long) with each injection. On examination the patient appeared healthy and had the physique of a well-developed bodybuilder. He had mild pyrexia (38.2°C). The left gluteal region was erythematous, hard and tender to palpation. A contrast-enhanced CT scan was requested to evaluate for the presence of a drainable abscess. This revealed a large inflammatory mass involving the left gluteal area (Fig. 1a).
The mass involved both the gluteal musculature as well as the adjacent subcutaneous tissue. There were also punctate and linear areas of calcification involving the gluteal muscles on both sides in keeping with the history of multiple injections over a long period to these areas (Fig. 1b).
In addition, several small lobules of low attenuation were detected within the gluteal muscles bilaterally. These were of fat attenuation ranging from –4 to –20 HU (Fig. 1c).
The patient was admitted and treated with intravenous antibiotics (Cloxacillin1gram IV, four times daily for 5 days). This failed to reduce the patient's symptoms and further imaging with ultrasound and MRI was arranged. Ultrasound examination was performed using a linear 5-MHz probe. This showed a large inflammatory mass with foci of calcification. No evidence of frank abscess formation was seen.
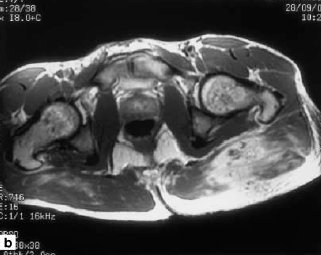
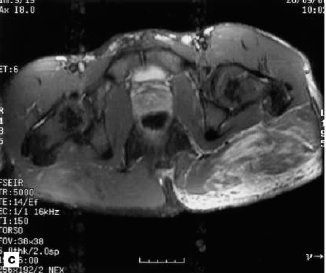
Magnetic resonance imaging at 1.5 T (GE signa, General Electric, Milwaukee, Wis.) of the lesion was then performed utilizing an imaging protocol consisting of transverse T1-weighted sequences (TR=716 ms, TE=16 ms), pre- and post-IV gadodiamide 0.5 mmol/ml (Omniscan, Nycomed, Oslo, Norway), as well as transverse short tau inversion recovery (STIR) and coronal fast spin-echo T2 (TR=4000 ms, TEeff=85 ms) sequences using a phased-array torso coil. This again demonstrated an inflammatory mass with evidence of mild enhancement post gadolinium (Fig. 4b, 4c). Areas of fat and calcification were again identified in both gluteal regions correlating to the previous CT findings.
As no drainable abscess was detected, the patient was again maintained on clindamycin 450 mg three times daily and ciprofloxacin 500 mg twice daily for 2 weeks with limited response.
The patient eventually has surgical debridement of the mass as well as intraoperative biopsies. Ziehl-Neelsen stains of the biopsy specimen showed acid-fast organisms and the surgical pathology demonstrated hypertrophic epidermis with the underlying dermis showing prominent perivascular and interstitial necrotizing granulomatous change. Positive identification of a mycobacterial organism took several weeks (Mycobacterium fortuitum).
During this period the patient was treated with clindamycin 450 mg three times daily, and ciprofloxacin 500 mg twice daily, and made an uneventful recovery. The patient was discharged and on follow up had made an almost complete recovery.
|
|
|